
Forget the endless lists of key success factors for change. The one thing that determines the success of a change is a tapestry composed of a 1000 hands. That’s what I experienced first-hand.
Today and the day before yesterday it went well. We could enter the vein without any trouble and the flow was good during the complete injection. That’s a big relief, because for the last three weeks we had a lot of trouble finding the right spot, locating the vein and simply entering it. It was so frustrating to have to try a second and a third time and sometimes needing to go to the hospital again to let us help.
That’s when his tears start rolling. It’s beyond frustration. It’s a defeat, and it’s hard in those moments to look our son straight in his tear-stained eyes and say: I’m sorry, it just doesn’t seem to work today and we don’t want to hurt you any more than this.
So here we are; back at the point that we need the nurses to go over every detail with us once more. Only to find out that we are doing it correctly and that in their presence it all goes so smooth.
We are literally dangling between the stage of conscious incompetence and conscious competence. A humbling experience.
Being a Target
Last summer my wife and I were put in the driver’s seat of a change that impacts our daily lives seriously.
Our son was born with a genetic bleeding disorder, called hemophilia A, which causes him to bleed longer than other people. In order to prevent serious bleeds we need to give him clotting factor every other day. But clotting factor is a substance that cannot be prescribed orally since it is digested before it reaches the blood.
When he was diagnosed, he was still a baby and the medical team implanted a port-a-cath device under his skin. This is a small box that is directly attached to the blood system. For years it allowed us to perform the injections through a small cushion the size of a pea. This is a procedure that is easy to perform; you can’t miss it.
But now our son is growing older and the port-a-cath was removed in order to switch to intravenous injections. We knew that this would be coming sooner or later. It means that we need to become skilled at giving intravenous injections.
To our own nine-year old son…

Take that in for a second. All of a sudden we found ourselves in the target position of a change.
Numerous times I go through the cycle of change with my clients, we analyze target behaviors, carve out strategies and coach people. And now I realized that it has been a long time since I went through that cycle myself.
In a very short time we were going to be skilled at giving intravenous injections and the training we received the next days made it all very tangible: my wife and I got to try it out on each other, on ourselves and even on the nurses who trained us.
Change Leadership
In just a few days we needed to take ownership of this thing. Although we were very determined to master intravenous treatments, the feeling of vulnerability was overwhelming at certain moments. I remember saying to myself: ‘Ahh, so this is what conscious incompetence feels like’.
We knew that we needed to take ownership of this change, because after all that’s what we do for a profession, right? It took courage, vulnerability and perseverance from our end… you know, the classic key success factors for a successful change, right? I could even throw in some ‘change leadership’ to top off the story: diving in head-first and without hesitation… yes to that as well.
My wife and I formed a solid team and acted on the problem like a textbook example of a change effort: Sounds fantastic, doesn’t it? What could possibly go wrong when you have courage and leadership?
What if I told you that those key success factors were not that decisive in us taking ownership of the change? They were necessary, but far from sufficient. There is something else that has played a major role in our taking ownership of the change.
1000 Hands
As you can guess, this is just half the story. Stopping here doesn’t do justice to all the elements that contributed to us taking ownership. Here is what really made a difference.
As my wife and I went through this change we always felt as if a 1000 hands carried us from the very beginning: the nurses, the doctors, the psychologists, the school, our friends, our family. All of them supported us since the diagnosis. And all of them were there to support us during this change.
Since the diagnosis 9 years ago, the bleeding disorder blended in to our daily lives and we were only reminded of it when there was an incident or when someone heard about it for the first time. Each time someone told us “But that must be hard.” we’d be answering “Yes, but it’s kind of part of our life.” I guess that’s how it goes with most disorders and disabilities. It becomes part of your unconscious competence skill set. But most of all: you begin to take those 1000 hands for granted.
Then, there is a crack in the egg, you become the vulnerable target of a change and you literally wake up to the fact that you are being carried by those 1000 hands. Those 1000 hands; that’s our community. But that community of 1000 hands doesn’t come together in a split second. It’s a fabric that builds over time and its delicate threads are the relationships of trust and bonding between people.
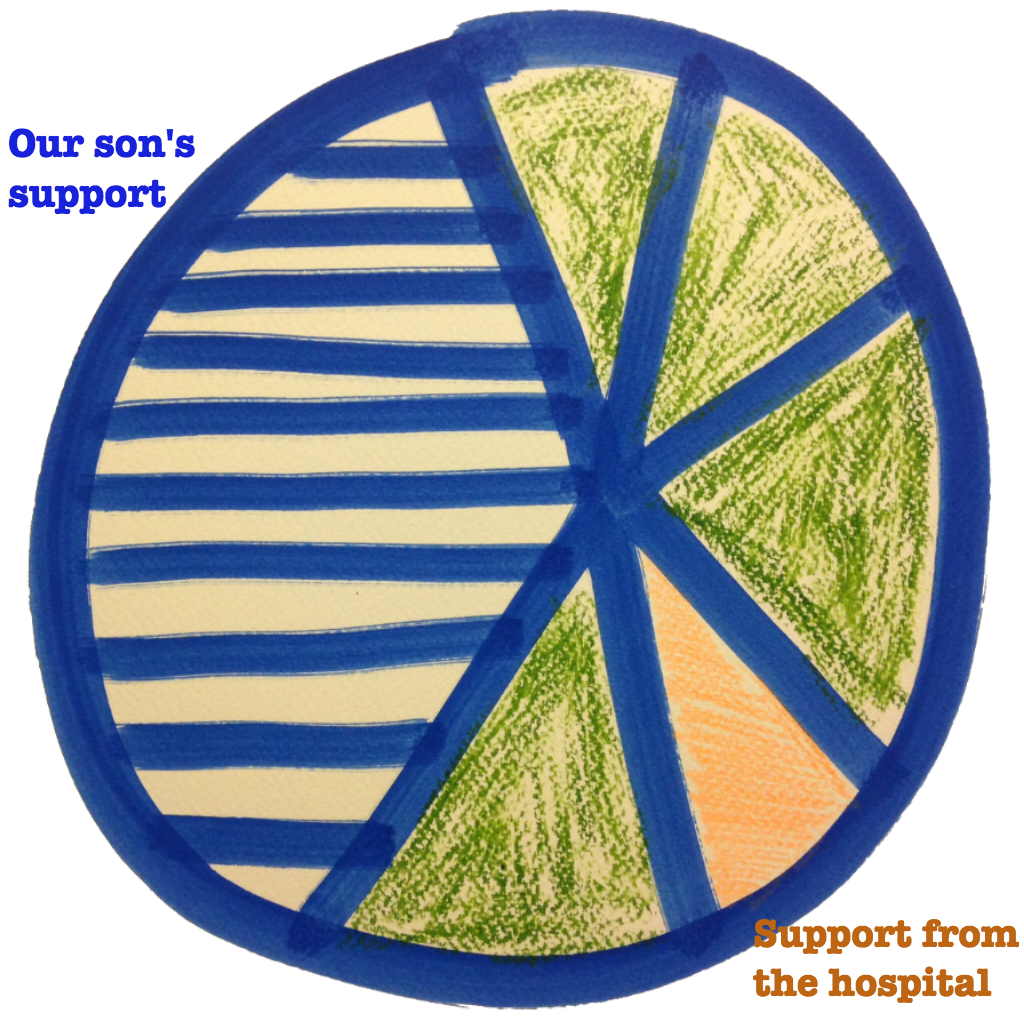
Let’s take a closer look at the tapestry of 1000 hands and examine how that fabric is composed. If we were to draw a pie chart of the 1000 supporting hands, the largest part would be taken up by the support we felt from our son.
I remember the first time I needed to perform the intravenous shot on him I was hovering back and forth between the table and the couch because the light was not good enough for me to see his veins. It took me more than 10 minutes of wrestling in my discomfort to ‘get it right’. And then he paused me, took me by the hand, looked me in eyes and said: “It’s going to be OK dad.”
At that point I wondered: in a care-giving situation, who is carrying whom? The last time I asked myself that question was when my mother passed away. That was 15 years ago. For a long time she went through a series of incorrect diagnoses, wrong treatments and hard battles against cancer before she finally had no strength left. She had to let go. And yet, during that long period of fighting and letting go it always felt as if she was carrying our whole family.
We had lost all faith in the doctors and the medical staff. We felt completely on our own. And this made her part of the heavy lifting even more tangible. Until her last breath we felt mentally carried and supported by her.
Have another look at that question: who is carrying whom in each stage of that emotional rollercoaster? During her work with terminally ill patients Elisabeth Kuebler Ross found that they typically come to terms with their prognosis in five stages: denial, anger, bargaining, depression, and finally acceptance. Since 1969 her insights have been fundamental for our profession to describe the stages of a change and the best way for practitioners to respond. Yet, we automatically assume that it is the practitioner and not the client who is doing all the work.
We fail to see that most of the capacity for change resides in the context instead of the practitioner “leading” the change.
3D-glasses
The truth is that people are not healed by a healthcare system, but by a tapestry of ‘thousand hands’. And sometimes it seems like the harder we look the more the sight gets blurred. Like watching a 3D movie without 3D-glasses.
Imagine a pair of glasses for looking at this situation that would offer sharpness and access to an extra dimension. We would have a clear and sharp understanding of the possibilities that are present in the context. We would respond differently to the hands that are reaching out to us, because we would see them for what they are: potential allies instead of undefined and blurred threats.
Let’s take this one step further and look back at the insights of John McKnight when he explains the difference between service and care. An organization like a hospital delivers a service. We pay medical staff and the social security system in order for them to provide us service. But people do not heal from service alone.
- The goal of an organization is to service its clients at the best possible ‘service’ level (be it in terms of operational excellence, product leadership or customer intimacy). A service is something you pay for. It is retribution-based;
- A community is capable of producing ‘care’. You cannot pay for care. Care is a commitment from the heart from one person to another.
The service of a hospital and the care of a patient community are two layers of the same reality that are connected to the health of a patient.
There is No Outside
We often refer to the difference between ‘service’ and ‘care’ as ‘formal’ versus ‘informal’. Others would refer to this difference as “command & control” versus “community”. And before you know it we have ended up in an animated movie with good guys and bad guys. But service and care are part of the same tapestry, they are just different layers.
There is no outside. This is what we do when we address Social Architecture: we discover the layers that have always been there and we integrate those that have been blurring our sight all along. For instance, in the case of our son:
- We feel supported by our son, who is the very target of this care-situation;
- We are serviced by a layer of hospital services;
- We are connected to the digital Facebook group called Hemophilia Mom, that connects us to other parents with the same challenges;
- Our son is connected to other kids with hemophilia through a yearly camp that is organized by the patient community;
- We feel supported by our family and friends who can comfort us and help us out when needed;
- etc.
This list goes on and it is composed of both: very formal task-oriented layers (‘service’) and other layers that are purely relationship-based (‘care’). The question is not whether one layer is better than another, but rather how well they can be accessed by the targets / clients of the initiative.

The better we are connected to all of those layers, the more we will feel responsible over our situation.
Ownership resides in the layers of care. They are characterized by relational and community dynamics, rather than command-and-control structural dynamics. In the previous post of this series I have underscored that both layers need to co-exist in the same way as a skeleton is a perfect structure to keep muscles, tissue and organs into place.
- Community-layers are the tissue and the muscles that tie the skeleton together.
- Command-and-control is the skeleton helps to keep muscles, tissue and organs into place
I concluded by saying that this is not an ‘either/or’ game; rather it is an ‘and/and’ situation. Both systems need to be switched on at the same time and all of the time. We get in trouble when one of them drops. This was the case with the situation of my mother’s struggle fifteen years earlier.
In the particular situation of my mother’s disease we felt very isolated and disconnected from all other layers. All potential for ownership was replaced by helplessness because our sight was simply too blurred. Over time helplessness turns sour and turns into a sense of entitlement. Eventually entitlement is what makes us blind for the different layers of community. It’s a negative self-fulfilling cycle.
The Road of Making Sense
Imagine how we felt when we were in the professor’s office the first time we discussed the diagnosis of our son’s disorder. With the previous experience of my mother’s journey in our backpack the level of trust in the medical system was very low and our helplessness had turned sour long time ago. This was not a good place to be in.
Fortunately the professor and the medical team were humble enough to try to understand where we were coming from. They granted us the time to come to terms with this diagnosis. They never argued or denied our previous bad experiences with the medical system. The access to a layer of belonging (community) was slowly opening up.
It was clear from that first visit that this was going to be a long-term partnership and that we had some work to do to get out of our helpless position of entitlement. This is when the true work of sense-making began for us. Making sense of the diagnosis, making sense of the help that was offered, making sense of the impact this all had on our lives. And there it was: a fork in the road:
- We could either choose to stick to the entitlements of service and increase our own sense of isolation and helplessness. This equals the child-role in a parenting relationship.
- Or we could choose to connect to the hands reached out to us by the different layers that were becoming visible to us. This results in a partnership.
Because seriously… it’s a choice. And those layers become visible and accessible at the speed of making sense.
Unlocking the Potential
It’s starting to dawn on us that the way we look at our situation – the 3D-glasses we have put on – is the key success factor that determines our ownership of the change.
We can see the hands that are reaching out to us; we connect to the different layers and if there is one thing blurring right now, it’s the difference between the formal and the informal layers as we have become a thread of the tapestry connecting the layers.
One thing is clear to us: we are holding the key to unlock the potential of the layers. That’s where it starts: with us.
